Normal Structure of Dentin
 |
| (A) Scanning electron micrograph of etched dentine showing exposed collagen fibres. Superficial collagen has been dissolved by collagenase to remove the most superficial collagen fibres that were damaged by tooth preparation. (B) higher magnification shows the characteristic collagen banding in inter-tubular collagen. |
Pathology of Dentine Caries
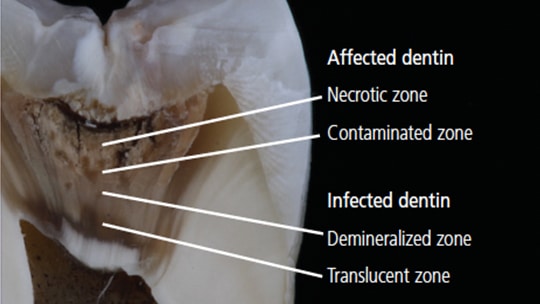 |
| Zone of carious dentine |
Dentine infection is facilitated by the dentinal tubules, which form an open path for bacteria, once they have been slightly enlarged by acid attack. After demineralization, the dentin matrix is gradually destroyed by the proteolytic enzymes secreted by the bacteria.
Streptococci play the main role in attacking enamel, but bacteria on the advancing front of the dentin forms a diverse flora of facultative anaerobes and anaerobes. Commonly isolated species include Lactobacilli, Actinomyces, Bifidobacterium, and Eubacterium, with S. mutans in varying amounts, the latter probably contributing to faster progression. The flora is proteolytic and more dependent on the dentin matrix for nutrients than dietary sugars.
Decalcified dentin initially retains its normal morphology. Once the bacteria reach the enamel junction, they spread along the tubules, quickly fill them, and spread along all the side branches. Tubules spread from the expanding masses of bacteria and their products, that the softened matrix cannot confine. Subsequently, the walls of the intermediate tubules are destroyed and the collections of bacteria in the adjacent tubules combine to form irregular foci of liquefaction. These, in turn, combine to induce progressively more extensive tissue destruction. Eventually, the dentin is completely destroyed. In some areas, cracks filled with bacteria form at right angles to the general direction of the tubules. Clinically, these cracks can allow the excavation of carious dentin in fragments in a plane parallel to the surface.
Caries in dentine, therefore, presents areas of demineralization, bacterial penetration, and destruction of dentin. The degree of destruction of dentin is essential for restorative treatment. Even in the area of bacterial penetration, much of the dentin structure is intact and can remineralize. It is, therefore, possible to restore a tooth leaving cavities and bacteria under the restoration, provided that the restoration is of high quality and obtains an adequate adhesive peripheral seal. No bacterial substrate can, therefore, reach the bacteria, the caries process stops and the dentin can remineralize.
The dentinal caries is then divided into areas, caries affected and caries infected. Dentine affected by caries is demineralized and its matrix is only partially degraded; part of the tubular structure remains and the number of bacteria is low. On the contrary, the area infected with caries, clinically identifiable as soft, wet, and brown, is largely demineralized, has no intact residual matrix to remineralize, tubules do not remain intact; and become spindle shaped laden with bacteria and its product. The area infected with caries cannot remineralize effectively and provides little support for restoration. It usually needs to be removed.
Protective reactions of dentine and pulpal caries
The spread of caries in dentin is considerably slowed down by a series of defense reactions mounted by vital dentin and pulp and mediated by odontoblast activity. These reactions are nonspecific and can be caused by other irritants such as friction, erosion, abrasion, and restorative procedures. The dentin changes begin even before the cavity forms in the enamel, but it takes time and is, therefore, more likely to grow prominently under the slowly progressing caries. Dentin is deposited by the original odontoblasts, both as peritubular dentin and pulp. Once the odontoblast dies, defense reactions within the dentin cannot occur, but reactive dentin can form. This is a faster response of odontoblast-like cells which differentiate from pulp cells, are possible as long as the pulp is not devitalized. The changes in dentin start to develop early, but at best, they can only slow the progression of tooth decay. Densely mineralized translucent dentin is also vulnerable to bacterial acid and proteolysis, and once bacteria enter normal dentin, they can invade the reactionary and reparative dentine to reach the pulp.
Ref:
- Cawson's Essentials of Oral Pathology and Oral Madicines 9th Ed.
- https://decisionsindentistry.com/article/clinical-treatment-of-deep-caries/