Clinical and Histological Features of Dental Caries
Now we shall describes the clinical features of carious lesions on smooth,
occlusal, and root surfaces. We shall relate the clinical features to their histological
features. We shall consider Enamel and Dentine together, the reasons being:
As a clinician, you will see them in the same way.
You can not understand changes in dentine during caries progression and caries arrest without considering the spread of the enamel lesion.
Changes in Dentine occur before the enamel lesion cavitates. Removal of the biofilm will arrest the lesion in dentine as well as the lesion in enamel.
The lesion, in both enamel and dentine, entirely reflects the activity of the bacterial biofilm.
Before I start talking about the clinical and histological features of dental caries, You must know the
Basic Structure of Enamel
Sound enamel consists of crystals of hydroxyapatite packed tightly together in an orderly arrangement which is known as enamel prisms. The amount of hydroxyapatite ranges between 86 to 95%; the organic component between 1% to 2 % and water between 4% to 12% by volume. The total inorganic content of enamel ranges between 95% to 98% by mass, thats why it looks like crystals.
The crystals are so tightly packed that the enamel gets a glass-like appearance and appears translucent. This is the reason that it allows the varying degrees of yellow colour of the dentine to shine through it. Here, you should know that even though the crystal packing is very tight, each crystal is actually separated from its neighbours by tiny intercrystalline spaces or pores. These spaces are filled with water and organic material. When enamel is exposed to acids produced in the microbial biofilm, mineral is removed from the surface of the crystal which shrinks in size. Thus, the intercrystalline spaces enlarge and the tissue becomes more porous. This increase in porosity can be seen clinically as a white spot.

Fig 1. Early enamel caries of maxillary central incisors as white spots on labial surface in the cervical area
Fig 2. This photograph shows enamel microstructure as a schematic diagram of keyhole-shaped enamel prisms or rods about 5 μm in diameter (B). Atomic force microscopy (AFM) images showing prism cross sections in A and along axes of the prisms in C. Crystallite orientation deviates in the inter-rod and tail area, and the organic content increases in the inter-rod area. (Ref: 2. The Oral Environment )

Histopathology of Enamel Caries
At this stage to help you understand better, I shall explain about the enamel caries. The early enamel lesion that appear as chalky spot or white spot on smooth surface below contact area are distinctly divided into four zones at histological level. These zones are, starting from dentino enamel junction towards enamel surface are
Translucent zone
Dark zone
Body zone
Surface zone

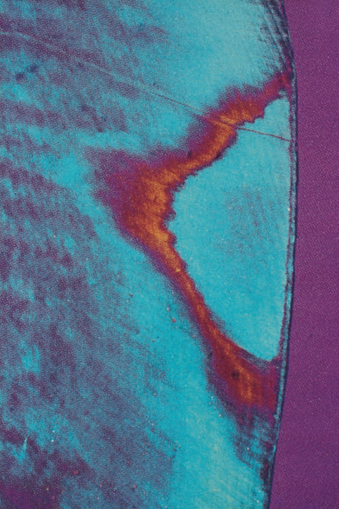
Fig 2. This photograph shows early enamel caries. The ground section is being viewed by polarised light after immersion in quinoline. Quinoline has filled the larger pores, causing most of the fine detail in the body of the lesion to disappear but the dark zone with its smaller pores is accentuated.
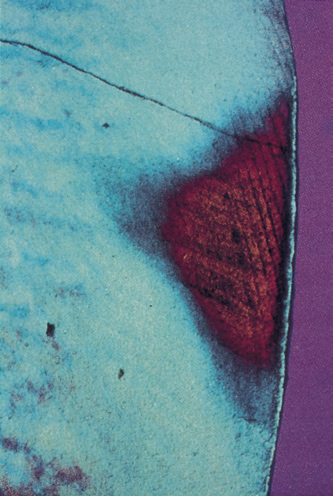
Fig 3.Photograph also shows early enamel caries. The ground section is being viewed by polarised light after immersion water. The body of the lesion and the intact surface layer is visible. The translucent and dark zones are not seen until the section is viewed immersed
in quinoline.
In the translucent zone, there is 1% mineral loss. This is the earliest and deepest demineralisation. It is broader in progressing caries but narrow or absent in arrested or remineralised lesion.
In Dark zone, there is 2%–4% mineral loss overall but a zone of remineralisation
just behind the advancing front will be present. This zone is broader in arrested or remineralised lesions, but narrow in advancing lesion.
In the body zone, there will be 5–25% mineral loss. It is broader in progressing caries which is replaced by a broad dark zone in arrested or remineralised lesion.
In the surface zone, there is 1% mineral loss. A zone of remineralisation is present that results from the diffusion barrier and mineral content of plaque. Cavitation is loss of this layer, allowing bacteria to enter the lesion. It has relatively constant width being a little thicker in arrested or remineralising lesions.
What is the clinical significance of this piece of knowledge?
It is important to know the histopathology of enamel caries as this knowledge will help you in preventing the further progression of the carious lesion into the dentin. Once you know about enamel caries, you can adopt preventive measures to revert back the situation thus not allowing the cavitation of the enamel. You can suggest plaque removal techniques like proper tooth brushing, flossing, antibacterial or fluoride mouthwashes or even you can go for professional fluoride application if patient or the guardian in cases of minor patient consent for it.
MCQs
Ref: