Bacterial lesions causing ulcerative conditions in the oral cavity
- Syphilis
- Gonorrhoea
- Tuberculosis
- Leprosy
- Actinomycosis
- Noma
For paid courses, a detailed description of the bacterial infection of the oral cavity is given HERE.
You must know the properties of the materials used in dentistry to understand its function and how and why it works in oral cavity. It also helps in manipulating it. The main properties you should know about are following:
Enamel: This is the hard, calcified substance that makes the surface of a crown of a tooth.
Pulp: This is the organ at the centre of a tooth that contains blood vessels, connective and neural tissue, and cells that produce dentine-odontoblast. Blood vessels and neural tissue enter the tooth from the apex of the root.
Periodontal ligament: This is the ligament that connects a tooth, by its root, to the supporting bone.
Cementum: This is the calcified tissue on the surface of the root of a tooth, which provides attachment for the periodontal ligament.
Fissure: It is a naturally occurring crevice in the enamel.
Crown: This is the part of the tooth that is visible and is above the gingival margin.
Root: This is the part of the tooth below the gingival margin; it is connected through cementum on its surface and the fibres of the periodontal ligament to the supporting bone.

There are numerous dental numbering systems to identify teeth and their
maturity. The most commonly used system in Australia is the Federation Dentaire
Internationale (FDI) system
The FDI numbering system divides the mouth into quadrants. The first
number indicates the quadrant and whether it is a primary or secondary tooth.
The second number indicates the tooth; tooth numbering begins at the central
incisor and counts backward to the molars.
Using the FDI numbering system, for adults, the quadrants are numbered as:
1. patient’s upper right is quadrant 1
2. patient’s upper left is quadrant 2
3. patient’s lower left is quadrant 3
4. patient’s lower right is quadrant 4

For primary teeth in children, the quadrants are numbered as:
1. patient’s upper right is quadrant 5
2. patient’s upper left is quadrant 6
3. patient’s lower left is quadrant 7
4. patient’s lower right is quadrant 8

 |
| Face bow-for Whip mix Arcon articulator |
Face bow is a device that is used to transfer the relationship of upper jaw to the temporomandibular joint and the skull. The use of face bow are as follows:
 |
| Face bow for Hanau Non-Arcon Articulator |
Dens invaginatus, dens in dente or tooth with in a tooth is a rare developmental anomaly. In it, the lingual pit is extended deep in to the crown or root, in later instance causing pulpitis. It is mostly seen in the maxillary lateral incisors but may be found in any anterior tooth.
 |
| Dens in Dente-lateral incisors |
 |
| A. showing Type I Dens Invaginatus in lateral incisors. Note- periapical cyst. B. Type II dens invaginatus in second premolar and C. Type III dens invaginatus in mandibular canine. [1] Ref:
|
The 2017 ACC/AHA guideline for high BP in adults provides four BP categories based on the average of two or more in-office readings on 2 or more occasions:
Even though they are benign and slow-growing lesions, ameloblastomas exhibit locally destructive behavior with a high recurrence rate. Thus, most relapses (50% and even over 80%) occur during the first 5 years after the primary surgery. The major contributing factor for recurrence seems to be the inadequate initial surgical procedure rather than the histological type [1].
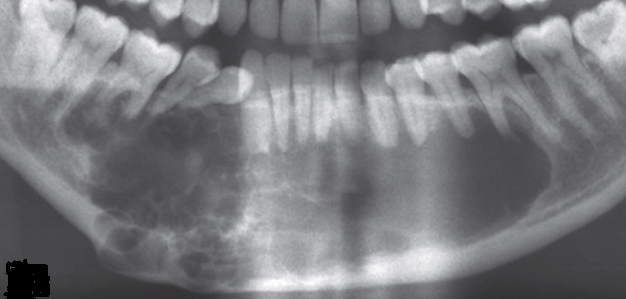 |
| Fig. 1. Ameloblastoma: multilocular appearance |
The surgical options for ameloblastoma vary from simple enucleation (with or without bony curettage) to radical excision.
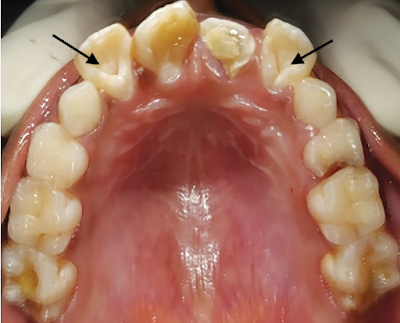
Extra numbers of teeth are known as supernumerary teeth. When they are present in the anterior maxilla in midline, they are known as mesiodens. When the extra teeth are present in the molar region as fourth molar, they are known as paramolar teeth. The anterior midline of the maxilla is the most common site whereas the maxillary molar area is the second most common site for supernumerary teeth.
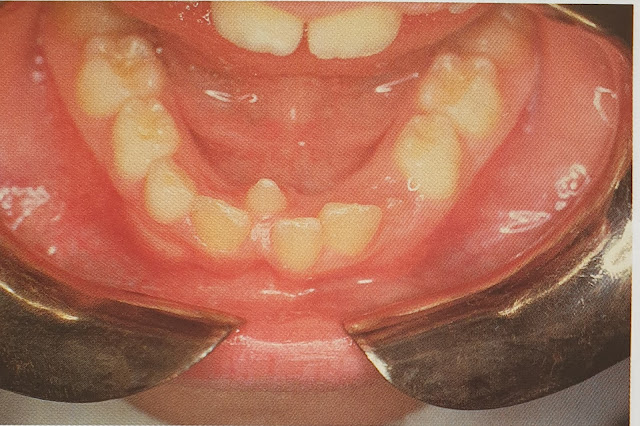
Supernumerary tooth-mesiodens in anterior mandible in midline [1]
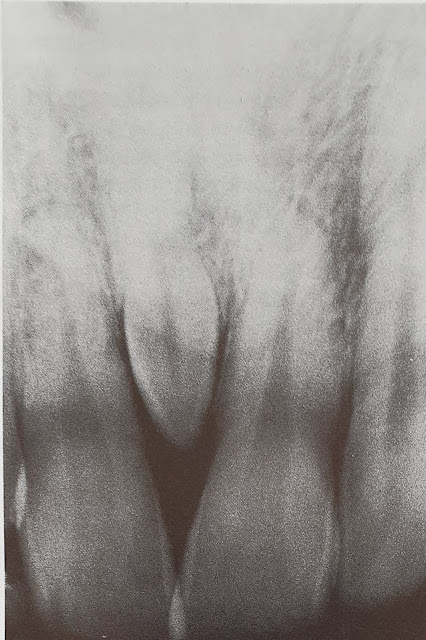
Radiograph showing mesiodens in anterior maxilla [1]
The investigation involves routine blood examination and IOPA or OPG radiographs. Depending on the anticipated level of difficulty of the surgery, additional investigations may be advised.
Treatment involves surgical extraction.
Oral candidiasis is a fungal disease that is caused by Candida albicans. It looks like a white or creamy plaque or patch that can be wiped off with the help of a cotton swab or a tooth brush leaving a red base.
 |
| Gingival thrush |
It occurs due to disturbance in the oral microflora due to antibiotics, corticosteroid, Xerostomia , immune defects especially in HIV infection, immunosuppressant, leukaemia or lymphomas and diabetes. It rarely occurs in a healthy individuals except in neonates.
 |
| Chronic mucocutaneous candidosis: note the wide adherent plaque. |
Gram stain smear shows the Candida albicans hyphae. It should be differentiated from Koplik's spot or Fordyce's granules.
The treatment involves treating the cause. Antifungal agents, for example, nystatin oral suspension or pastilles, amphotericin lozenges, or miconazole gel or tablets or fluconazole tablets can be given.
Ref:
1. Oral diseases 2nd Ed. Crispian Scully, Roderick A. Cawson Churchill Livingstone
MALOCCLUSION
Proposed by Edward H. Angle in 1890, the Angle Classifications are based on the relationship of the buccal groove of the mandibular first permanent molar and the mesiobuccal cusp of the maxillary first permanent molar. This classification is considered to be one of the most commonly used as its easy to use.